Based on clinical evidence in regards to NSAIDs:
Patients should, avoid NSAIDs before and after PRP treatment to ensure optimal results.
Dawn Michelle Lipscomb, PhD, is a biophysicist, podcast host, and science writer. While finishing a dual B.S. in Physics and Biology at UT San Antonio, she published research on planetary biosignatures for space exploration at NASA-JPL and designed THz bioeffects experiments for human tissues at the Air Force. In 2017, she completed her Biophysics doctorate at UC Berkeley by developing a new method for imaging human proteins that regulate gene expression using cryo-electron microscopy Today, she co-hosts a live video podcast series on regenerative medicine and writes articles about groundbreaking research in aging and genetics.
There is significant debate in the field of orthobiologics regarding effective protocols for platelet rich plasma (PRP) treatments. PRP therapy has rapidly emerged as an effective regenerative therapy for musculoskeletal conditions, sports injuries, cosmetic tissue repair and a promising alternative to surgical intervention. At a cursory glance, the medical literature reveals conflicting results, which merits a critical scientific review. Effective scientific study designs and clinical success depends upon a deep understanding of the therapeutic process and the ability to sort out variables in study design, such as; preparation method, dosage, activation, administration techniques, and now controlling for the inhibitory effect of non-steroidal anti-inflammatory drugs (NSAIDs) on platelet aggregation. According to recent research, NSAIDs negatively impact the healing potential of PRP therapy by reducing platelet function.¹
In 2016 researchers at the Clinical Center for Sports Medicine & Orthopaedic Surgery and the Medical University of Graz, Austria designed an experiment to test the effects of NSAIDs on platelet function. The study utilized light transmission aggregometry to assess the platelet function of PRP prepared from two unique groups. The study group included 11 patients taking NSAIDs (dexibuprofen, 400 mg or diclofenac, 75 mg) twice daily for and average of 3.2 days prior to PRP preparation. The control group consisted of 10 healthy volunteers without history of NSAID use during the two weeks prior to PRP preparation.
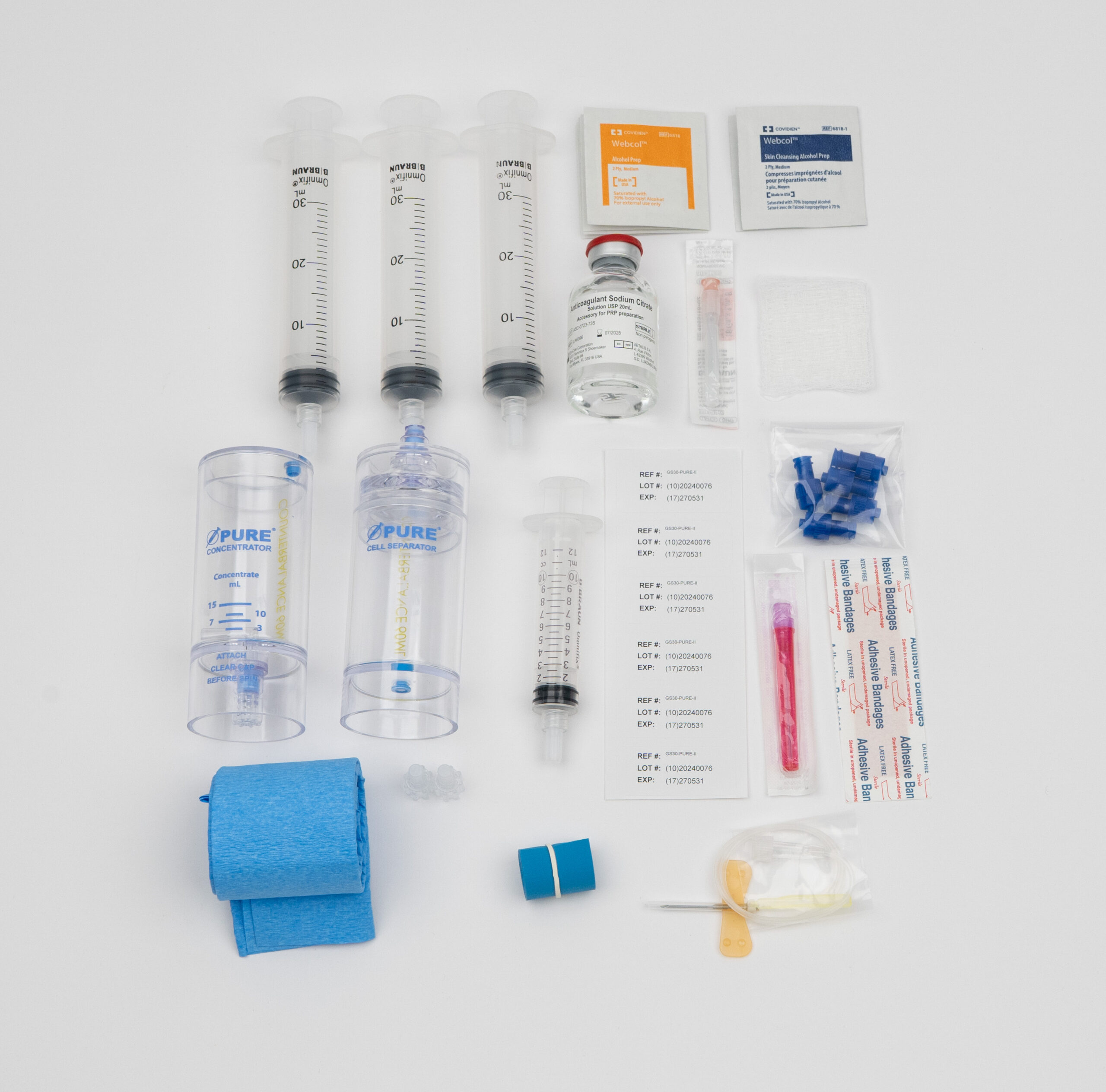
In both groups, researchers used two distinct commercially available systems to prepare PRP; a dual spin kit and a kit designed to yield PRP from a single centrifugation. By preparing PRP on multiple platforms, the study controlled for the influence of preparation method on platelet viability. The researchers prepared PRP according to manufacturer’s guidelines and then analyzed platelet counts of all serums with a hematological analyzer. They found no significant difference in platelet count between groups or across platforms.

The researchers assessed platelet viability by stimulating 450 µL of PRP with 4 standard inductors of platelet aggregation, including; thrombin receptor–activated peptide–6 (TRAP-6; 20 µL), collagen (1 µL), adenosine diphospate (ADP; 5 µL), and arachidonic acid (AA; 5 µL). Outcomes were assessed with light transmission aggregometry (LTA) which quantifies changes in turbidity (or cloudiness) with an optical detection system. LTA is commonly used to detect platelet disorders and the effect of antiplatelet medication² as changes in turbidity are proportional to platelet aggregation.
The researchers recorded a statistically significant difference in platelet function in samples stimulated with arachidonic acid in the NSAID group. Platelet stimulation from TRAP-6, collagen, and ADP showed little difference between the control and study group. This statistically significant difference appeared in both PRP kits and whether patients were taking dexibuprofen or diclofenac.
Arachidonic acid is a fatty acid used across clinical research to assess platelet aggregation and the effect of NSAIDs on platelet function. A burst of oxygen is released when arachidonic acid is combined with PRP in vitro. This influx in O(2) triggers platelet aggregation through the the phospholipase A2-cyclo-oxygenase–thromboxane A2 pathway, wherein arachidonic acid is converted into cyclo-oxygenase stimulating platelet aggregation. The use of NSAIDs reduces cyclo-oxygenase–mediated oxygen consumption which in turn reduces platelet aggregation, degranulation and growth factor release.¹
All PRP preparation techniques start with a blood draw into the presence of an anticoagulant. The anticoagulant prevents platelet activation during the mechanical force of centrifugation. If platelets activate during the preparation process, a blood clot will form and the resulting serum will have platelet concentrations no higher than whole blood. Additionally, a serum prepared without an anticoagulant would not contain the beneficial growth factors central to effective PRP therapy. Activation releases growth factors which are tiny proteins that would rise to the surface of the supernatant, if platelets are prematurely activated.
In the aforementioned study, both preparation techniques utilized 3.8% sodium citrate concentrate as an anticoagulant, which controls for the potential influence of various anticoagulants on platelet function. The use of different anticoagulants effects the resulting PRP. A 2016 study out of Brazil found that PRP prepared with sodium citrate as an anticoagulant yielded serums with higher platelet concentrations compared to PRP prepared with citrate dextrose solution A or ethylenediaminetetraacetic acid.³
Why Arthrex ACP Did Not Show Significant Improvement: Several factors could contribute to the lack of significant improvement. These include the inherent variability in PRP compositions, differences in patient populations, and the placebo effect. Additionally, the study’s setting in a real-world clinical practice may introduce variability that is not present in more controlled environments.
Comparison with Previous Studies on PRP Effectiveness: Previous studies on PRP have shown mixed results. Some randomized controlled trials (RCTs) have reported significant benefits, while others have found minimal or no improvement. The inconsistencies across studies highlight the need for standardized protocols and a better understanding of patient selection criteria.
Examination of Potential Variables: The study explored various patient factors such as age, sex, BMI, Kellgren and Lawrence grade, and history of knee trauma. None of these factors were found to predict clinical outcomes, indicating that the effectiveness of Arthrex ACP may not be influenced by these variables. This suggests that other unexamined factors or a combination of factors could play a role.

Rudimentarily, platelets function to stop bleeding whenever the vascular wall is ruptured. If the vascular wall is ruptured, collagen present in subendothelial tissues initiates a clotting cascade. Platelets bind to collagen directly via the glycoprotein (GP) receptor complex. After binding, collagen receptors on the platelets initiate phospholipase C-mediated cascades. This leads to an increase in intracellular calcium which initiates morphological changes in platelet structure (such as the presentation of pro-coagulant surfaces) and the secretion of platelet granular content (ie growth factors).⁴ Researchers utilized LTA to assess platelet aggregation because platelet aggregation and degranulation go hand in hand. Platelet degranulation is the release of bioactive growth factors which initiate a healing cascade at the site of PRP injections. Platelet aggregation is an indicator of healthy platelet functioning and a prerequisite for degranulation. The presence of NSAIDs disrupts this process by inhibiting cyclooxygenase which interrupts arachidonic acid aggregation while indirectly inhibiting collagen stimulated aggregation.
NSAIDs are a class of analgesics which block cyclooxygenase (COX). COX is an isoenzyme which produces prostaglandins, thromboxane, and levuloglandins. Prostaglandins support platelet health, protect the thinning of the stomach and induce inflammation as part of the healing cascade. By reducing prostaglandins, NSAIDs reduce inflammation and therefore pain. Consequently, the use of NSAIDs is also associated with stomach bleeding and reduced platelet health.
NSAIDs are the standard household pain reliever and were once commonly prescribed to reduce the risk of heart attack. Though common knowledge still assumes aspirin thins the blood and reduces heart attack, researchers in Montreal confirmed the opposite in 2017.⁵ After pooling patient data from 61,460 myocardial infarction events in the elderly population (over 65 years), the study found current use of NSAIDs significantly increased the risk of heart attack.
Though Canadian researchers found evidence contradicting the use of NSAIDs to prevent heart attack, these analgesics are still commonly used to reduce pain and inflammation for athletes and patients with arthritis. The mechanism of action which makes NSAIDs effective pain relievers also inhibits platelet aggregation via the cyclooxygenase-arachidonic acid pathway. This means that PRP prepared while patients are taking NSAIDs will not achieve therapeutic potential because platelet function is impaired.
Without proper aggregation, platelets won’t be able to release growth factors such as platelet derived growth factor, vascular endothelial growth factor and transforming growth factor beta, among others. These tiny bioactive proteins are at the heart of successful PRP therapy. They promote tissue regeneration by direct surrounding cells to increase mitogenesis, chemotaxis and angiogenesis.⁶ As such, patients who abstain from the use of NSAIDs for two weeks prior to PRP preparation will benefit from increased platelet function and growth factor release.

Daniel Zengel, an executive with over 10 years of experience in the pharmaceutical and medical device space, is dedicated to delivering industry-leading, cost-effective products to US-based medical providers. Specializing in regenerative medicine, Daniel focuses on sales, training, and marketing support to help clinics across the country successfully implement platelet-rich plasma (PRP) therapy.