Hip osteoarthritis (OA) is a degenerative, wear and tear, condition that affects about one in ten Americans. The condition dramatically decreases quality of life by making everyday activities such as walking, sitting, standing and laying difficult and painful. Growing elderly populations have increased interest in the search for effective hip osteoarthritis treatments. Hyaluronic acid (HA) injections and platelet rich plasma (PRP) injections are among the most promising therapies because of decreased risk of systemic side effects. This article discusses the efficacy of PRP injections for hip OA based on the clinical evidence available.
Researchers from the Rizzoli Orthopedic Institute in Bologna compared the effects of PRP and HA injections and published their findings in 2016 in the American Journal of Sports Medicine.¹ The study design included 111 patients with hip osteoarthritis at a pain intensity greater than >20 on a 100 mm visual analogue scale (VAS). Patients were divided into three groups. Each group received 3 weekly intra articular injections of either PRP (44 patients), HA (36 patients), or PRP with HA (31 patients). Patients in the HA group received 2ml of Hyalubrix 30 mg/2 mL and the HA + PRP group received 5 ml of PRP + 2 ml of HA.
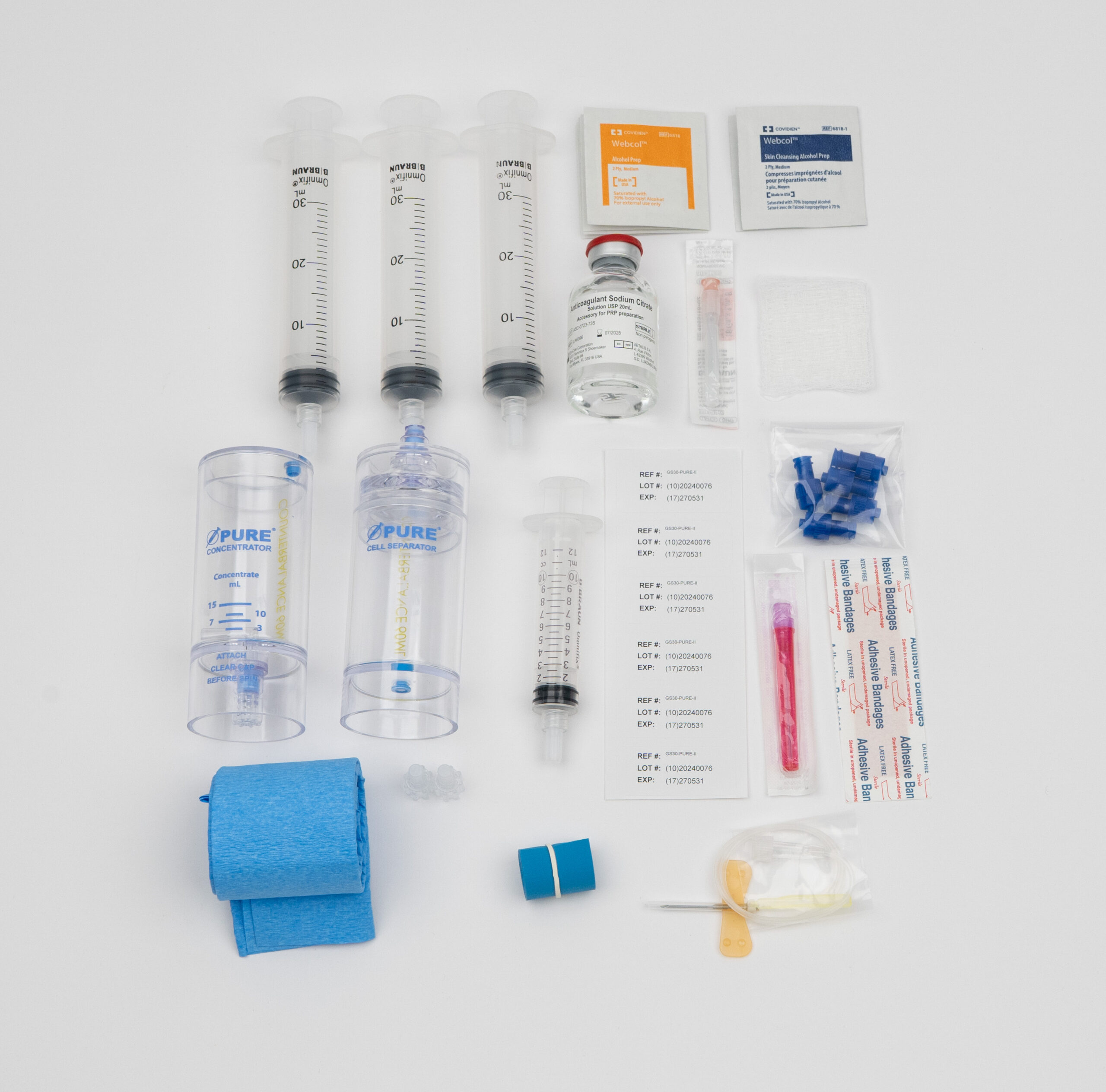
PRP was prepared from 150 or 300 ml of peripheral blood (150ml in unilateral cases and 300ml in bilateral cases). The sample was centrifuged at 1480 rpm for 6 minutes and again at 3400 rpm for 15 minutes to yield 4 or 7 aliquots of PRP, each 5 ml.
One in four PRP samples (PRP group: n = 13; PRP+HA group: n = 8) were analyzed with human enzyme-linked immunosorbent assay kits (Boster Immunoleader) for the following proinflammatory and anti-inflammatory markers:
Outcomes were assessed with the visual analogue scale (VAS), the Harris Hip Score (HHS), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Patients were assessed at baseline and again 2 months, 6 months and 12 months after the last injection.
The study found WOMAC scores in the PRP group significantly improved at 2 & 6 month follow-up. Researchers also noted a ‘‘moderate’’ correlation between interleukin-10 and variations of the VAS score. Overall PRP injections alone were found to be more effective than HA injections.
Previous studies have shown PRP to reduce pain and enhance function in osteoarthritis of the knee.² The damaged osteochondral tissue in hip OA is benefitted by growth factors released during platelet degranulation. Growth factors are tiny bioactive proteins which are known to promote growth of the extracellular matrix. The extracellular matrix provides the scaffolding for chondral tissue to regrow and catches migrating stem cells. Growth factors can also modulate inflammation, promote healthy vasculature, and lend to the body’s ability to create hyaluronic acid for joint lubrication. By increasing mitogenesis in chondral tissue and lubrication, PRP injections could potentially stop the progression of hip OA, while decreasing pain and increasing mobility.
In 2017 researchers in Sassari, Italy compared PRP injections with HA and found statistically significant improvements in both groups.³ The study included 80 participants ages 40-72 with early hip OA. PRP was prepared by drawing 150 ml of venous blood. Then spinning the sample as with a dual centrifugation method; first at 1,480 rpm for 6 minutes, then at 3,400 rpm for 15 minutes to concentrate platelets. (Note: the previous study used peripheral blood: are peripheral blood and venous blood the same thing?) From 150ml of whole blood the process yielded 20ml of PRP, which was divided into (4) 5ml portions. Three were administered through weekly intra articular injection and one was sent to the lab to assess platelet concentration and quality. Patients in the HA group received Hyalubrix 15 mg/mL (Fidia; Abano Terme, Italy).
The results were assessed with the same outcome measures as the aforementioned AJSM study (VAS, HHS, WOMAC). The researchers found a statistically significant reduction in WOMAC pain scores in both groups at the 6 mo and 12 mo follow up, but no statistical difference between groups.
Differences between study design and PRP preparation can easily influence the final results. Neither study mentioned which commercially available PRP kits were used. There are wide differences between the composition of the final PRP preparation depending on which kit is employed, how accurately the manufacturer’s protocols were followed, and the initial composition of the patient’s blood. Disparity between kit can lead to diverging results. Third party analysis has shown that some products produce PRP with platelet concentration half that of whole blood, while others produce PRP 7x more concentrated that whole blood.⁴
To control for some of these differences, researchers should employ lab tools to assess the composition and potency of the final product. The later study failed to assess growth factor content of PRP, which may have revealed how differences between kits and individual biochemistry influences PRP potency. While it may be impractical in a clinical setting, additional lab work will increase replicability of research and help to elucidate the complex relationships between PRP and healing.
Additional limitations:
Future studies should include analysis of the patients whole blood and the final PRP serum for platelet concentration and growth factor release. This information is fundamental for the replication of results and a deeper understanding of outcomes.
Hip OA is the number one reason for total hip replacement, and surgical intervention is on the rise. For example, total hip replacement increased 63% across Canada from 1999-2009.⁵ There is a huge need for interventions that halt and reverse the progression of osteoarthritis. If the condition is caught promptly, early treatment options include intra-articular HA and PRP injections. Osteoarthritis progresses as intra-articular levels of HA decrease. Decreasing HA levels lower the viscoelasticity of synovial fluid and increases articular friction. Simple HA injections can delay surgery and improve joint lubrication in the short term, but require regular follow up injections. Intra-articular PRP injections increase the body’s capacity to produce HA by increasing proliferation of the chondral cells which produce HA. Based on our review of the current literature, PRP significantly improves outcomes for patients with hip OA and offers more long term benefits when compared to HA injections.

Daniel Zengel, an executive with over 10 years of experience in the pharmaceutical and medical device space, is dedicated to delivering industry-leading, cost-effective products to US-based medical providers. Specializing in regenerative medicine, Daniel focuses on sales, training, and marketing support to help clinics across the country successfully implement platelet-rich plasma (PRP) therapy.