Knee osteoarthritis is a degenerative condition that affects about 20 million Americans. As we age, the activities of daily living slowly wear away the articular cartilage of our knees. Once cartilage deteriorates, it is difficult for the body to repair. Generally, tissue repair depends on healthy blood flow, but cartilage is nonvascular tissue which receives nutrients via synovial fluid. Traditional treatment methods aim to manage pain and prevent surgery, while making little attempt to repair cartilage. Cartilage repair is possible with platelet rich plasma injections. The regenerative potential of PRP gives new hope to those suffering with knee osteoarthritis by injecting beneficial growth factors right where the body needs them.

Obesity is a common risk factor for knee osteoarthritis because of the added mechanical stress to the knees. For every extra pound of weight we carry, 4 pounds of pressure are added to the knees.¹ Women suffer from knee osteoarthritis at a significantly higher rate than men. Though researchers have yet to elucidate the factors that put women at higher risk, hypothesis point to anatomical differences that influence joint articulation and hormone changes in postmenopausal women.² Athletes and manual laborers show an increased incidence of knee osteoarthritis attributed to the gradual accumulation of micro-traumas from high impact sports and consistent occupational stress.
Weight loss is often the first treatment option recommended if indicated. This relieves pressure and has been shown to relieve pain when paired with moderate exercise.³ Other first line traditional treatment options include nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, hyaluronic acid injections and physical therapy. Unfortunately, studies have found little evidence to support the use of NSAIDs to treat knee osteoarthritis, which makes sense because inflammation does not appear to be the primary driver of deterioration in osteoarthritic knees.⁴ Overall the etiology of knee osteoarthritis appears to be more mechanical than biological. Though some researchers have started to explore the relationship between obesity, knee osteoarthritis and inflammation related to the metabolism of lipid and glucose.⁵
Though a corticosteroid injection may offer immediate, short term pain relief, overall these injections lead to unfavorable outcomes. A recent long term study shows corticosteroid injections actually increased cartilage loss without decreasing pain over a 2-year period.⁶ Alternatively, hyaluronic acid increases the viscosity of synovial fluid and occurs naturally inside the intra-articular space. The body manufactures this compound to lubricate the joint. Studies have shown hyaluronic acid injections to be minimally effective in treating knee osteoarthritis, with more favorable results for high-molecular weight injections. Beyond injections, physical therapy can be helpful to align joint articulation by selectively strengthening surrounding muscles. In advanced cases, total knee replacement surgery may be the only option.
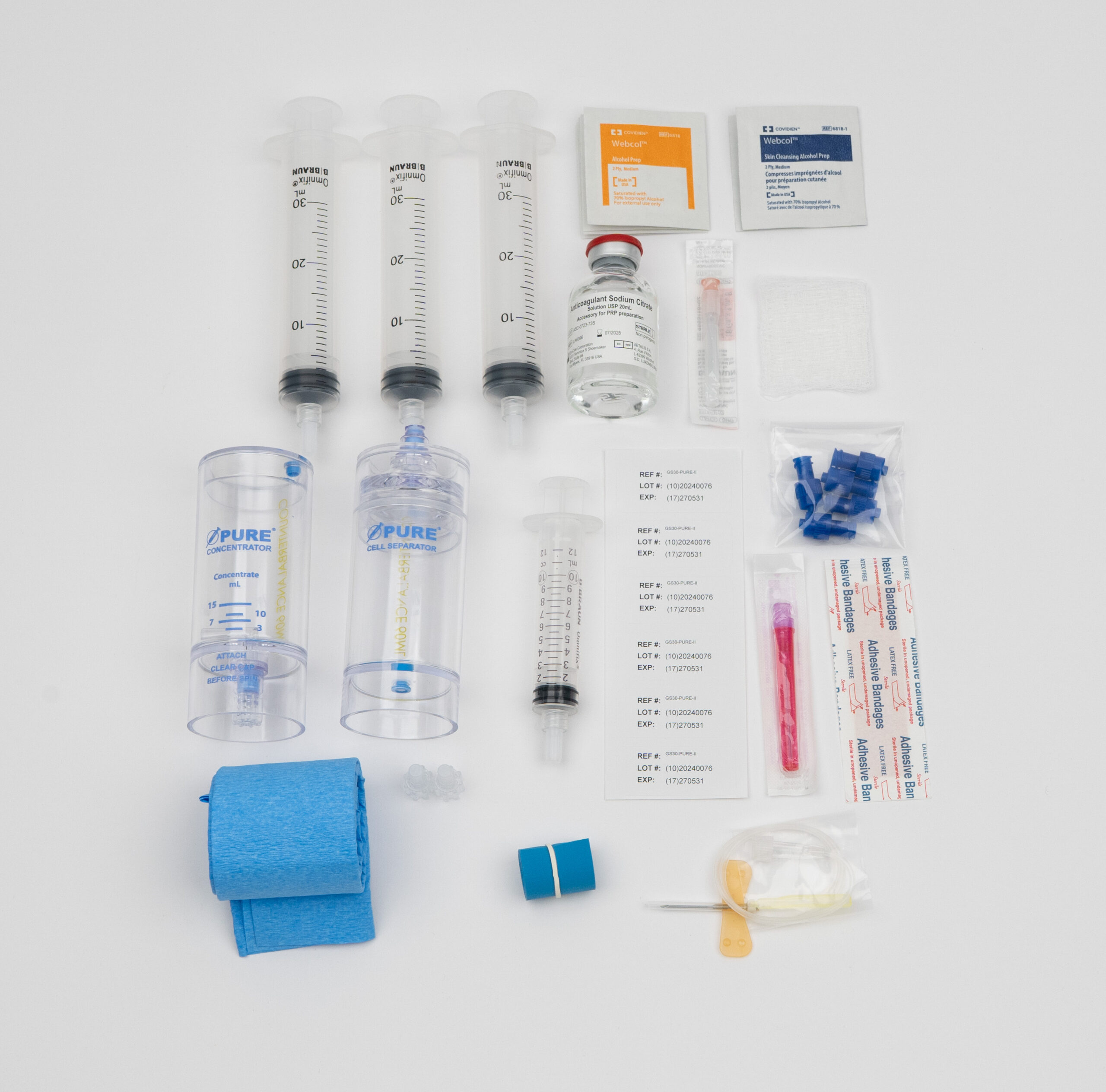
Physicians aiming to improve outcomes for patients with knee osteoarthritis are beginning to integrate intra-articular platelet rich plasma injections. A 2013, level I study completed by researchers in India found PRP injections to be more effective than placebo. A total of 156 knees were divided into three groups; group A received a single injection of PRP, group B received 2 PRP injections 3 weeks apart, and group C received a single saline injection. Platelet rich plasma injections were prepared from 100 ml of whole blood, yielding 10 ml of pure PRP (leukocyte free). Assessed outcomes included the Western Ontario and McMaster Universities Arthritis Index (WOMAC), joint stiffness, physical function, pain and patient satisfaction. Researchers found statistically significant WOMAC score improvements and significant pain reduction in both groups treated with PRP.⁷

Researchers in Tehran published a year long study comparing the effects of platelet rich plasma injections and hyaluronic acid in osteoarthritic knees. One hundred sixty patients were divided into two groups; 87 participated in the PRP group and 73 in the HA group. In the PRP group, 4-6 ml of leukocyte-rich PRP was prepared from 35-40 ml of whole blood. Patients received 2 injections of PRP at a 4 week interval. The HA group received 3 injections of high-molecular-weight hyaluronic acid each one week apart. Researchers looked at WOMAC scores and general health according to SF-36 surveys (patient-reported assessment of physical and mental wellbeing) and found PRP to be more effective than HA injections. Patients receiving PRP injections had better outcomes with increased functionality and quality of life scores.⁸
Platelets contain over 30 growth factors involved in healing damaged tissues throughout the body. The purpose of PRP therapy is to concentrate these regenerative growth factors then deliver them directly to damaged tissues. Connective tissue growth factor (CTGF) and fibroblast growth factor (FGF) are of particular interest for osteoarthritic applications of PRP. Both CTFG and FGF promote cartilage regeneration via the proliferation and differentiation of chondrocytes.⁹ The regeneration of cartilage tissues with a biological product is a phenomenal advancement compared to the aforementioned traditional treatments.
The careful reader may notice how some researchers use leukocyte rich PRP preparations and others create pure PRP for intra articular injections. As this field advances it becomes more important for researchers to clearly define PRP preparation procedures so that results can be replicated. Investigators at Stanford University looked at the differences between leukocyte rich (LR) and leukocyte poor (LP) PRP for intra-articular joint injections and found more favorable outcomes with LP-PRP. LP-PRP activates more anti-inflammatory and fewer proinflammatory cytokines while still delivering an adequate concentration of platelets. Alternatively, LR-PRP showed less favorable outcomes for synoviocytes when compares to LP-PRP.¹⁰

Daniel Zengel, an executive with over 10 years of experience in the pharmaceutical and medical device space, is dedicated to delivering industry-leading, cost-effective products to US-based medical providers. Specializing in regenerative medicine, Daniel focuses on sales, training, and marketing support to help clinics across the country successfully implement platelet-rich plasma (PRP) therapy.