Dry socket is a painful post-operative condition that affects 25-30% of patients undergoing molar extraction. Dry socket or alveolar osteitis (AO) is characterized by severe, radiating pain which increases between the 1st and 3rd day after extraction. Without careful management, dry socket can lead to infection and jaw necrosis. Preventing dry socket is a high priority for oral surgeons, though most employ prevention strategies with little scientific underpinning. Successfully mitigating dry socket leads to better patient outcomes and decreased financial burden on the health care system. This article discusses recent research which found that activated platelet rich plasma (PRP) significantly reduced incidences of dry socket in high risk patients.
The 2017 study included 150 patients between the ages of 30-60 with increased risk for AO which included smokers, alcoholics, post-menopausal women, women taking oral contraceptives, and patients with pericoronitis (inflammation of the gums around a partially erupted tooth), or bruxism (teeth grinding).¹ The participants were randomized into 2 groups; group A included 75 patients who received activated PRP in the tooth socket after extraction. Patients in group B received standard care without the addition of PRP.

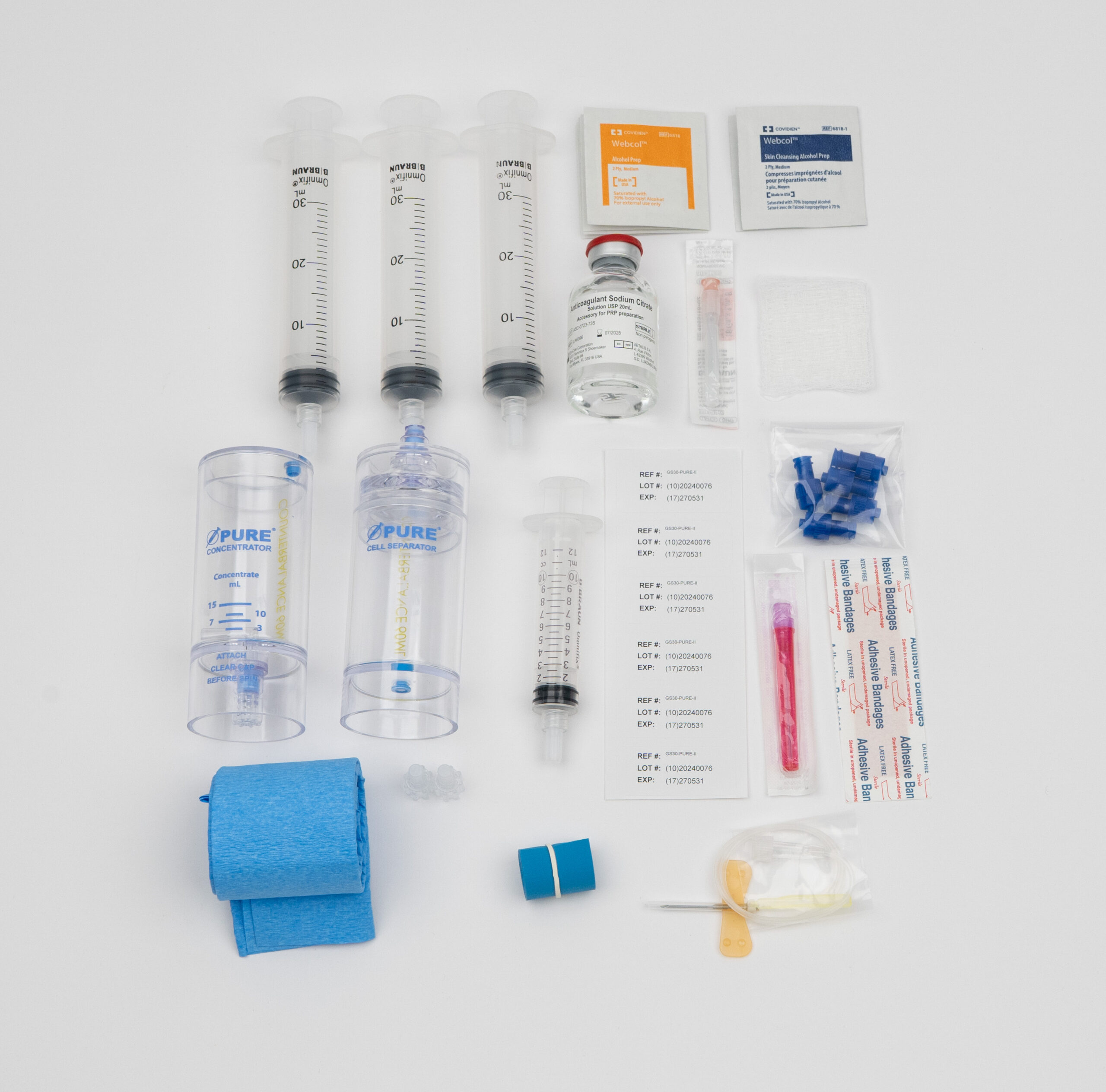
PRP was prepared by drawing a total of 8 ml of blood into 2 vacutainers each containing .5 ml of citrate-phosphate-dextrose with adenine as an anticoagulant. The mixture was centrifuged at 3000 rmp for 10 minutes to isolate erythrocytes (red blood cells) from platelet poor plasma (PPP) and the buffy coat (the thin layer of platelets and white blood cells directly above the red blood cells). The PPP supernatant, buffy coat, and top 1 mm of red blood cells were collected into a fresh vacutainer and then centrifuged at 4000 rpm for 10 min to further concentrate the platelets. The secondary centrifugation is an opportunity for more platelets to fall out of the PPP solution, which increases platelet concentration. The lower half of the secondary supernatant was thoroughly mixed and subsequently activated to yield a high hematocrit, leukocyte rich PRP. The final product contained about 3.5-4 times the platelet concentration of whole blood. Though this dose is sufficient for a therapeutic response, the use of a commercially available kit such as EmCyte Pure PRP would yield PRP with up to 7 times the platelet concentration.
Researchers activated the PRP with 0.5–1 cc of calcium chloride (CaCl₂) and left the serum undisturbed for 2–3 min. Adding CaCl₂ initiated platelet activation by lowering the pH and by introducing calcium which initiates a chemical chain reaction similar to in situ collagen activation. Platelet activation leads to degranulation, aggregation and the expression of growth factors as the platelets begin to coagulate into a gel.
Study participants were assessed for pain and dry socket on the 3rd and 5th day after surgery. At follow-up patients were evaluated for:
Results showed statistically significant reduction in incidences of dry socket in the PRP treatment group. The researchers found signs of dry socket in 12% of patients in the control group, while in only 1.3% of the treatment group showed signs of AO. Pain scores were assessed with the Wong-Baker visual analog scale on the 3rd and 5th day follow-up appointments. In addition to significantly reduced dry socket symptoms, patients in the treatment group experienced significantly reduced pain scores compared to the control group.
Persons with diminished circulation from smoking or taking oral contraceptives have an increased risk for dry socket because without proper blood flow, new tissue cannot regenerate. AO can also result from trauma to the wound site by the improper use of gauze or the pressure change from sucking on a straw. Even if these external risk factors are controlled, the initial clot can spontaneously dissolve due to increased fibrinolysis.² Fibrinolysis is a natural physiological processes in which fibrin is dissolved by plasmin at the site of injury and repair. Trauma to the alveolar bone during extraction converts plasminogen to plasmin which can dissolve the clot and lead to dry socket.
Alternatively, bacterial pyrogens can contribute to dry socket. A wide variety of bacterial strains thrive in the mouth. Bacteria such as treponema denficola secret pyrogens which convert plasminogen to plasmin and increase fibrinolysis (leading to dry socket). Thus the anti-bacterial properties of leukocytes contained in the aforementioned PRP gel preparation play a dual role in molar extraction healing; they help prevent bacterial infection and by reducing the potential for bacterial colonization, leukocytes downplay the potential for plasmin and fibrinolysis to dissolve established clots.

The healing power of PRP comes from applying a supraphysiologic concentration of platelets directly to damaged tissue. Platelets are the primary drivers of wound healing throughout the body. They are tiny fragments of megakaryocytes, large progenitors of hematopoietic stem cells located in bone marrow. During the final stages of maturation, megakaryocytes extend proplatelet elongations into sinusoidal blood vessels. The proplatelet elongations continue to mature inside the blood vessel and eventually release platelets into the bloodstream. They are just a fraction of the size of red blood cells and circulate through the blood at about 150,000 to 450,000 platelets per microliter of whole blood or about 1 trillion per adult.³
Platelets play an essential role in clot formation by changing shape, releasing alpha-granules and aggregating in response to blood vessel injury. Growth factors released during degranulation increase tissue regeneration by increasing cell mitosis, chemotaxis and stimulating angiogenesis. In the presence of a wound, as with the open socket left behind after molar extraction, growth factors signal to surrounding epithelial cells to increase proliferation.
Complete healing from tooth extraction requires the regeneration of soft tissue and, in many cases, bone. Postoperatively a healthy patient will regenerate connective tissue and osteoblasts as needed. Growth factors contained in PRP such as insulin-like growth factor, vascular endothelial growth factor, epidermal growth factor, nerve growth factor, transforming growth factor-β1&2, and platelet-derived growth factors rapidly increase the patient’s healing potential by increasing collagen production and vascular ingrowth at the surgical opening. Platelets also release cytokines such as angiopoietin-2 and interleukin-1 which notify surrounding and distant cells to migrate to the site of injury.
After extraction, filling the open tooth socket with activated PRP gel acts as a natural clot, but with the added benefit of growth factors and far superior adhesion. A natural blood clot is composed primarily of red blood cells with approximately 5% platelets and less than 1% white blood cells. The activated PRP gel forms a dense fibrin clot composed of 94% platelets, 5% red blood cells and approximately 1% white blood cells.¹
Even though there is significant evidence to support the use of PRP for many conditions, most stand alone PRP procedures are still considered ‘experimental’ by insurance companies. Fortunately many providers recognize the value of augmenting surgical procedures with PRP therapy and offer reimbursement for PRP with molar extraction. Given the proven potential for activated PRP gel to improve patient outcomes by reducing pain and incidence of dry socket, the addition of PRP therapy benefits all parties involved in standard molar extraction procedures.

Daniel Zengel, an executive with over 10 years of experience in the pharmaceutical and medical device space, is dedicated to delivering industry-leading, cost-effective products to US-based medical providers. Specializing in regenerative medicine, Daniel focuses on sales, training, and marketing support to help clinics across the country successfully implement platelet-rich plasma (PRP) therapy.