Platelet rich plasma (PRP) therapy and the bioactive proteins released after viable platelets are injected into degenerating or damaged tissues present an elegant combination of low risk with high potential for tissue regeneration.
PRP therapy is being applied in the field of embryology to help patients hoping to extend the window of fertility into perimenopause and beyond. This post examines the scientific evidence available to support the use of PRP injections for ovarian rejuvenation.
Since 1970, the availability of contraception as well as increasing education and economic opportunities have progressively delayed the onset of motherhood.¹ For some women the changing modern landscape and challenges of conception delay motherhood into perimenopause when ovarian function drops off rapidly. The desire to conceive in populations with declining ovarian function prompted a fertility clinic in Greece to experiment with PRP injections for ovarian rejuvenation.
In 2016, doctors at the Genesis Clinic in Athens presented a poster claiming the reactivation of folliculogenesis in perimenopausal women.² The abstract, presented at the European Society of Human Reproduction and Embryology meeting in Helsinki Finland, briefly summarized findings from 8 perimenopausal women. On average the subjects were 45 years old (+/- 4.4 years) and had experienced menstrual cessation for about 5 months prior to the PRP procedure. The authors claim that PRP injections temporarily restored ovarian activity.

Following whole blood centrifugation, the autologous serum was injected into the ovaries with guided transvaginal ultrasound imaging. Menstruation was observed 1-3 months following the procedure. Upon menstruation, all patients underwent the beginnings of natural in vitro fertilization (IVF)- without additional ovarian stimulation or gonadotropin-releasing hormone (GnRH) antagonist supplementation. Once a follicle greater than 16 mm was observed, ovulation was stimulated with 5000 IU of human chorionic gonadotropin (hCG) and follicle aspiration was conducted 32 hours later. The processes resulted in an average of 1.5 oocytes per patient which were artificially inseminated and cryopreserved for potential transplant at a later date.
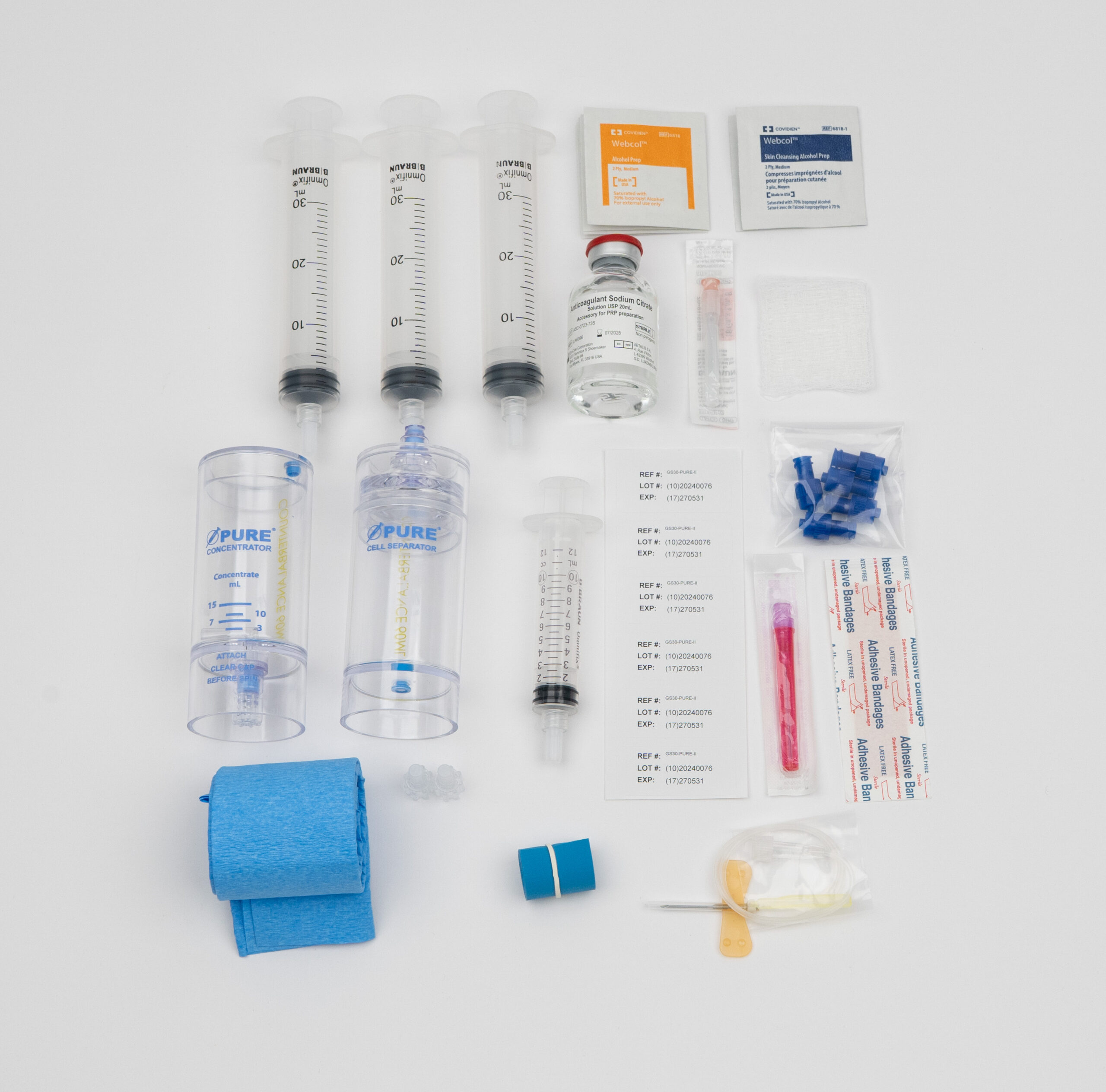
The authors provided little discussion of the PRP preparation process beyond mention of the use of gel separator kits. Luckily, PRP produced with gel based kits was analyzed in a study conducted by researchers at BioSciences Research Associates (BSR). BSR is an independent contract research laboratory located in Cambridge and once academically affiliated with Harvard Medical School.
Their analysis compared the efficacy of commercially available PRP kits and found that single-spin gel separator kits produced a serum with fewer platelets than whole blood.
According to the BSR results, regardless of the volume of the initial blood draw or serum injectate, the patients in the Genesis study were injected with a platelet poor plasma.³ Future ovarian rejuvenation studies would benefit from whole blood and PRP serum analysis in order to replicate PRP concentration and dosing.
The authors claimed the PRP injections stimulated ovarian rejuvenation, but are these claims well-founded? The menopausal transition is long and complex. Can we attribute folliculogenesis to the PRP injection or is sporadic ovulation normal in this population? To begin to answer these questions, let’s review what we understand about the menopause transition.⁴
Since 1996, Samar R. El Khoudary, PhD, MPH, FAHA, Associate Professor of Epidemiology at the University of Pittsburgh has been conducting a large and diverse, longitudinal Study of Women’s Health Across the Nation (SWAN). Over the past 23 years the study has tracked 3,302 women, documenting changes in mental health and physiological systems over the menopause transition. The data shows that natural menopause (defined as the lack of menstruation for 12 consecutive months) occurs just beyond the age of 50 for most women. Menstrual cycles begin to lengthen and the rate of ovulatory cycles slowly decrease an average of 7.5 years before the final period.
According to the average age of the participants and average length of time since their last menses, the women included in the Genesis Clinic abstract were in mid to late perimenopause as defined by the SWAN study. According to El Khoudary, the rate of ovulatory cycles begins to rapidly decline from 88% five years prior to the final menstruation down to 23% in the year before menopause. It’s not uncommon for ovaries to spontaneously ovulate after months of menstrual cessation; most women ovulate once during the final year of perimenopause.
It’s hard to know exactly what effect the PRP injection had on the participants because the abstract only included results related to ovulation.
Based on the information collected by El Khoudary and his colleagues, we can anticipate that women in mid to late perimenopause will continue to ovulate sporadically. Isolating the action of PRP injections might be possible upon reviewing data related to changes in follicle stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2) and anti-müllerian hormone (AMH).

With the limited data available, it seems premature to claim that PRP injections rejuvenate ovaries in perimenopausal women, though it’s certainly possible that PRP can play a role in reactivating declining ovarian tissue. For example, doctors at Genesis Clinic were prompted to examine the effectiveness of PRP injections on ovarian rejuvenation after reviewing a case-study published in the Journal of Ovarian Research.⁵
In 2013, the doctors at Hospital Sant Joan de Déu in Barcelona successfully re-implanted cryopreserved ovarian tissue into a 30 year old patient who’s ovaries had been removed 10 years prior after consecutive cystectomies.
Prior to transplantation, the doctors injected the preserved ovarian tissue with autologous PRP and relied on the angiogenic properties of growth factors (such as epidermal growth factor and connective tissue growth factor) to rapidly revascularize the tissue. Ovarian function was restored and spontaneous menstruation was observed 4.5 months after the procedure. The patient birthed a healthy baby boy with the help of ovarian stimulated in vitro fertilization.
Even with the potential for healing and limited risk for negative outcomes, it’s irresponsible to claim PRP injections rejuvenate ovaries without sufficient data. It’s important to remember this research has yet to be published in a peer-reviewed journal. The scientific process requires researchers to meticulously share their methodology, observations and measurements so experiments can be replicated. It seems curious that an endocrinology journal hasn’t picked up this first of it’s kind research.
Soon after this abstract was presented at the Helsinki Reproduction and Embryology conference, news of the potential for PRP to rejuvenate ovaries promptly spread across the internet.
During the same month of the 2016 conference, Konstantinos Pantos, the primary author and Chairman of the Board of Directors at Genesis Athens, was interviewed by the New Scientist.⁶ In the interview Pantos claims that he has injected 30 perimenopausal women with PRP and isolated and fertilized eggs from most of them. This information doesn’t align with the summary presented in Helsinki which stirs suspicions that the data presented in the abstract is skewed.
There is hope that more rigorous PRP-ovarian rejuvenation research will be shared in the future. Clinicaltrials.gov lists a study sponsored by Ascendance Biomedical that included 200 women over the age of 35 with amenorrhea lasting 3-6 months.⁷ The trial was designed to observe the effect of PRP injections on fertility outcomes in patients undergoing natural IVF.
Research team tracked FSH, LH, E2, AMH, progesterone and inhibin as well as changes in egg quality over a 12 month period. Results from the trial have yet to be released. Regrettably, the research team elected to use gel based kits, which yield a serum that is likely to include growth factors, but do not concentrate platelets into PRP.

Daniel Zengel, an executive with over 10 years of experience in the pharmaceutical and medical device space, is dedicated to delivering industry-leading, cost-effective products to US-based medical providers. Specializing in regenerative medicine, Daniel focuses on sales, training, and marketing support to help clinics across the country successfully implement platelet-rich plasma (PRP) therapy.