For nearly three decades, doctors have been observing the therapeutic effects of delivering a concentrated dose of autologous platelets to damaged tissues. Over the years, platelet rich plasma injections (PRP) have entered public consciousness and with increased demand, clinicians are looking for ways to provide quality PRP treatments that patients can afford.
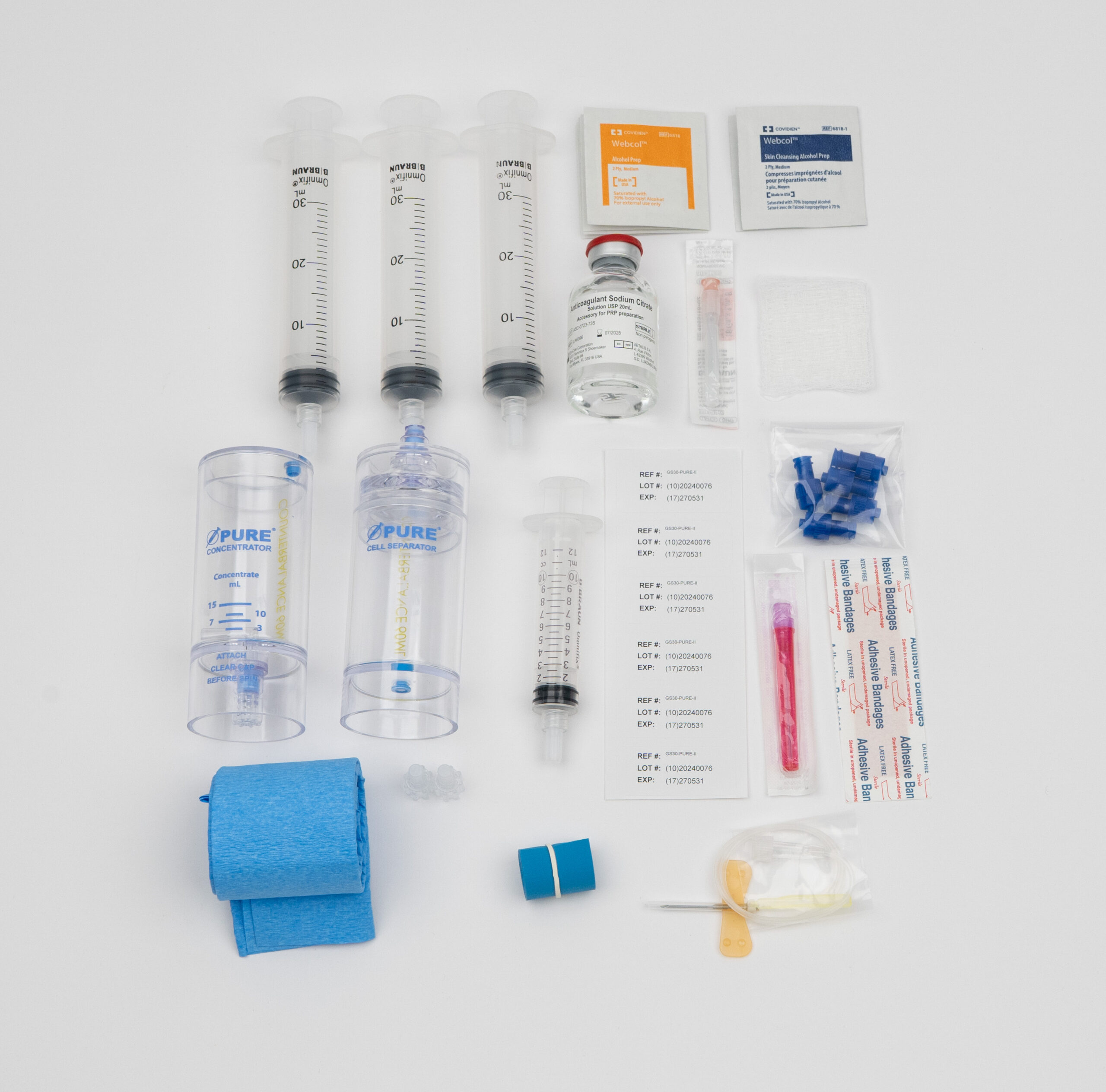
Commercially available PRP kits vary in their ability to adequately concentrate viable platelets, which leaves many doctors wondering if there is an opportunity to develop an in-house PRP preparation technique that doesn’t break the bank. This article examines two unique methods for preparing PRP serum outside of commercially available kits, and asks are homemade PRP preparation methods safe? Can they deliver a therapeutic dose of platelets? Are these in-house methods efficient?
The first study comes to us from researchers at the Izmir Education and Research Hospital in Turkey.¹ In 2014 Drs. Kececi, Ozsu, and Bilgir published research seeking to establish a low-cost PRP preparation method yielding standardized platelet concentration. The authors hypothesized that unsuccessful PRP treatment can be attributed to unrefined preparation methods with inconsistent platelet recovery rates.

First, the authors selected 18 volunteers between the ages of 22-50. The subjects were healthy without recent use of NSAIDs or other medications (for 10 days prior to blood draw). The researchers drew a total of 55 ml of blood from each patient in 6 separate vacuum tubes. Each vacuum tube contained 9 ml of the patient’s blood and 1 ml of 3.8w/v% sodium citrate solution, hermetically added with a 3-way valve to prevent platelet activation during the mechanical force of centrifugation. An 18 gauge needle was used to draw the blood in an attempt to minimize platelet trauma and activation. One milliliter of the patient’s whole blood was isolated for platelet analysis.
The PRP serum was prepared with two rounds of differential centrifugation. All samples underwent the same initial centrifugation or ‘soft spin’. The samples were spun at 250g for 10 minutes which isolated constituent blood particles by weight. Red blood cells, the heaviest blood elements, sank to the bottom of the vacuum tubes, followed by the buffy coat (which contains leukocytes and platelets) and topped with the remaining blood plasma (platelet poor plasma- PPP).
Next, the platelet poor plasma and buffy coat were aspirated into a new, sterile vacuum tube for secondary centrifugation. Dual centrifugation has become common practice and is used to further increase platelet concentration. During the force of the second centrifugation, more platelets precipitate out of the PPP. In this study researchers aimed to evaluate the effect of varying the force of the secondary spin on final platelet concentration. The samples of each participant were divided into 6 groups according to the force applied during secondary centrifugation from 300g up to 2000g for 10 minutes (with increments at 500g, 750g, 1000g, & 1500g).
ANOVA analysis revealed that platelet concentration increased with increasing g forces. There was no significant difference between the 300 & 500g groups, but platelet concentration increased significantly between 500g, 750g & 1000g centrifugation, and the average platelet count leveled off in the higher g-force groups with no significant increase from 1000-2000g.
While the authors deliberately articulate how the anticoagulant entered without potential for contamination, there is the larger concern of utilizing non-medical grade equipment to produce a serum meant for injection. The authors fail to list a brand or company associated with vacuum tubes so it is uncertain if the serum produced by these vacuum tubes could be safely injected.
Common blood lab materials; vacutainers, yellow tops, red tops and tiger top vacuum tubes and the like are not medical grade. These tubes may be a valuable resource in the blood lab and great for testing, they are not to be confused with medical equipment.
After the second spin, the top two thirds or 3 ml of PPP was gently aspirated leaving a final 1.5 ml of concentrated PRP. The authors determined PRP platelet count with repeated ANOVA (analysis of variance) tests and found all samples contained significantly higher platelet concentrations compared to whole blood. The serum analysis confirmed that their in-house method was successful in creating a platelet rich serum, but does this method yield a therapeutic dose of platelets?
There is plenty of research that shows PRP injections to be safe, improve wound healing and damaged tissues, but determining the exact therapeutic doses requires more large-scale clinical trials with adequate serum and growth factor assessments. It’s possible that certain tissues would respond to the platelet concentration yielded from the above methods (a secondary centrifugation-depended range from 500,000 to 975,000 platelet/µL), but therapeutic response is likely to depend on the tissues and damages in question.
For example, the serum acquired from the lower force secondary centrifugation may be ineffective for the treatment of osteoarthritis of the knee. In 2017 researchers at the Istanbul Kanuni Sultan Suleyman Training and Research Hospital assessed the therapeutic effects of PRP injections on patients with early stage-knee osteoarthritis. The study found a concentration of 1,000,000 platelets/µL to be therapeutic for pain relief and functional recovery. Secondary centrifugation of 750g or less yielded PRP with 725,000 platelets/µL, which may not be a sufficiently therapeutic dose.²
The authors acknowledged how conflicting results in the PRP literature could be linked to the wide variation in PRP preparation techniques. Non-standard preparation techniques and serum concentrations make inter-study comparative analysis challenging or impossible. The authors suggest that samples with lower baseline platelet counts could undergo higher secondary centrifugation while samples with higher baseline platelet counts could undergo secondary centrifugation at a lower g-force, which could result in a standard concentration across samples. The authors suggest that standardizing PRP serum concentrations would increase study comparability and lead to more predictable PRP outcomes.
The study shows how researchers could vary the force of secondary centrifugation to produce PRP serums with standard concentrations of platelets. While the process of varying secondary centrifugation based on blood analysis would be helpful in the realm of research, the time involved would make it impractical for clinical purposes.

The next method utilized common 5 ml syringes to produce PRP while evaluating the effect of anticoagulant dextrose solution A (ACD-A) and heparin on the presence of Platelet Derived Growth Factor BB (PDGF-BB).³ The researchers collected 60 ml of blood from two healthy volunteers (half was mixed with ACD-A and half with heparin at a 9 to 1 ratio). The researchers portioned 4 ml whole blood into 16 modified syringes and centrifuged at 3000 rpm (704g) for 3 minutes, the minimal amount to separate red blood cells. Next the researchers aspirated the plasma and buffy coat into another set of modified syringes via 3-way cock, half of which contained one microgram of prostaglandin E1 (PGE1) a platelet aggregation inhibitor. All samples underwent secondary centrifugation at 4000rpm (1252g) for 15 minutes. The supernatant was then discarded leaving .65ml of PRP in each syringe. Upon analysis, the researchers found samples prepared with ACD-A as well as PGE1 to yield PRP dense with PDGF-BB.
While this method utilizes readily available materials, it may not be practical in a clinical setting. Modifying common syringes presents abundant opportunity for human error and the introduction of pathogens. While it is novel to include a platelet aggregation inhibitor and helpful to assess platelet viability with PDGF-BB analysis, the process yielded a scant .65ml of PRP. Working with such small amounts of serum could make it difficult to deliver an adequate dose of platelets.
Developing an in-house process may be appealing to clinicians hoping to increase the availability of PRP treatments, but many potential downfalls come with homemade PRP. Injecting serums prepared with non-medical grade equipment has the potential to harm patients and risk licensure.

Daniel Zengel, an executive with over 10 years of experience in the pharmaceutical and medical device space, is dedicated to delivering industry-leading, cost-effective products to US-based medical providers. Specializing in regenerative medicine, Daniel focuses on sales, training, and marketing support to help clinics across the country successfully implement platelet-rich plasma (PRP) therapy.